The menstrual cycle is a (roughly) 28-day cycle controlled by female hormones.
The reason for the menstrual cycle is to prepare your body for a possible pregnancy. Your body goes through 4 phases each month, as an egg is released and is either fertilised (pregnancy) or broken down (a period). The timings of each phase differ slightly depending on what length cycle you have – cycle length can vary between women, and even month to month sometimes.
There are different levels of hormones interacting at each phase, and these can affect how you feel. Once you know what phase you’re in, you can work with your cycle to concentrate on activities that make the most of your mood, energy and general wellbeing.
The four phases of the menstrual cycle
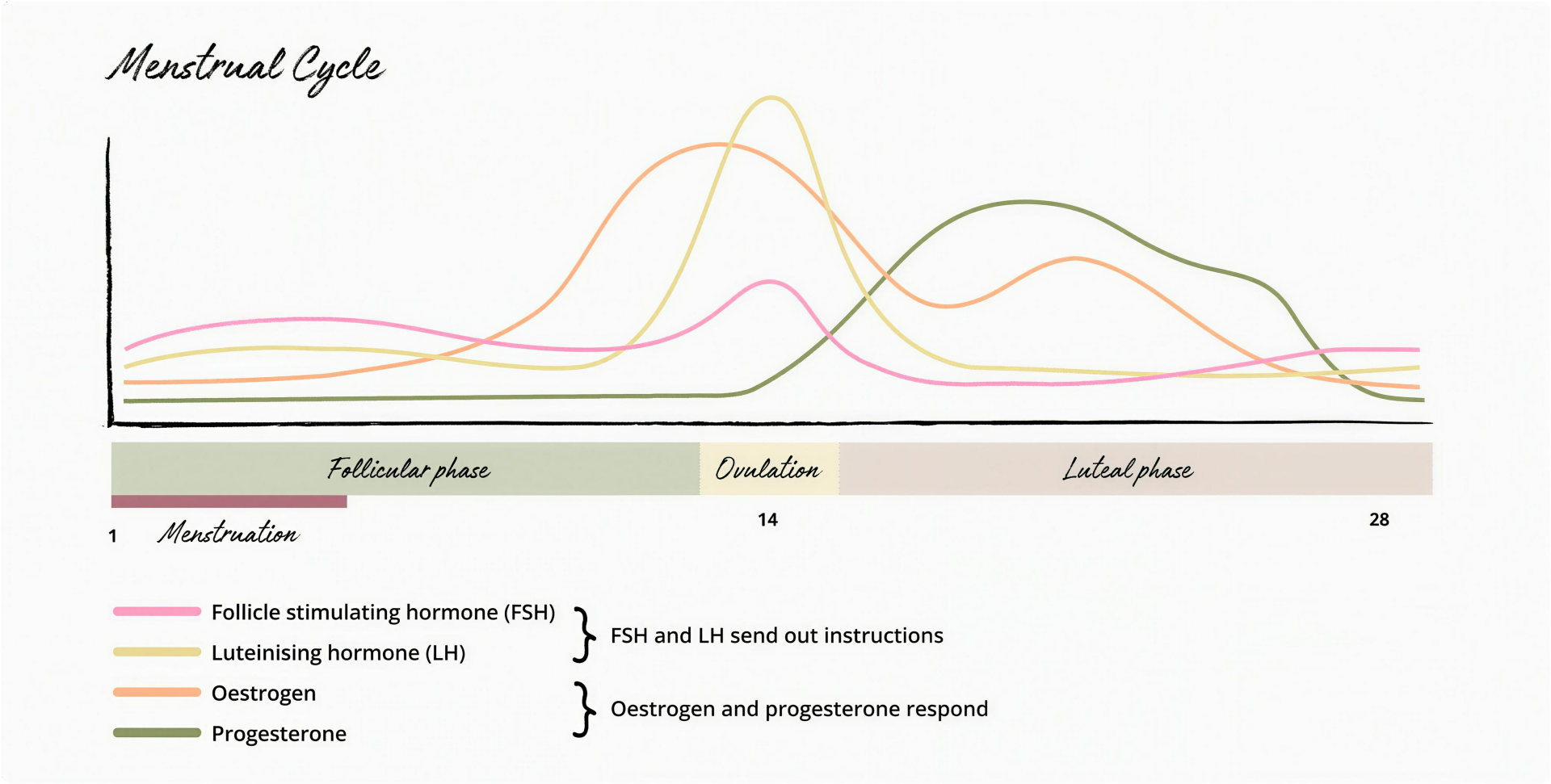
In each phase of your cycle you’ll experience rising or falling levels of four hormones. Hormones are like messengers, and are sent from one part of the body to another to tell it what to do. There are dozens of hormones in the human body, but the ones that matter most for your cycle are:
Menstruation - Day 1 (for up to a week)*
What’s happening?
Your uterus (womb) sheds its lining, and your Period starts. Periods usually last 3-7 days.
How do I feel?
As your hormones drop you may feel a little down or experience some mood swings.
Follicular Phase - Days - 13/14*
What’s happening?
Your uterus lining is thickening ready to receive an embryo. This phase crosses over with the Menstruation phase. The hormone FSH stimulates follicles in the ovary to grow. Usually only one follicle will mature into an egg (around day 10).
How do I feel?
Once your period is over you may feel like you have more energy; your brain feels sharper and your memory is better. You might have a higher pain threshold.
Ovulation - Day 14 (roughly)*
What’s happening?
A mature egg is released from the ovary and travels along a fallopian tube towards your uterus. It survives for 24 hours and can be fertilised if it meets a sperm during this time.
How do I feel?
For many women their positive emotions and feeling peak during this phase, and so does their libido.
Many women experience a higher sex drive during ovulation or at the end of this phase.
Luteal phase - Days 15-28*
What’s happening?
After ovulation progesterone is produced which thickens the uterus in preparation for pregnancy. If a fertilised egg implants into the uterus lining, this continues to be produced to maintain the thick uterus lining. If there is no embryo implanting, progesterone levels drop and the lining sheds, and your period starts.
How do I feel?
This is the phase you are most likely to experience PMS (premenstrual syndrome) symptoms such as mood swings and irritability. You may feel sluggish and absent-minded. Your sex drive may also drop, partly due to the high levels of progesterone, but also due to the other feelings you may be experiencing such as low mood or fatigue, which naturally makes you less interested in having sex!
*Timings differ depending on the length of the cycle
What is the ‘fertility window’?
The fertility window includes the days around ovulation where your chances of getting pregnant are highest. If you’re looking to conceive, it makes sense to time intercourse to fit in with your fertile window. Equally, if you do not want to get pregnant but are having regular sex with a male partner, it’s worth knowing when you both may need to be extra careful with your contraception.
Did you know?
It’s a myth that you can get pregnant at any point in your cycle. What IS true is that every woman is different, and each cycle is different, so it’s difficult to predict exactly when your fertile window will be.
What if I have irregular periods?
First off – you’re not alone. Many women experience cycles that change from month to month, and it’s estimated only 13% of women have a 28-day cycle. It’s completely normal to have cycles ranging from 25 to 30 days.
Your cycles can also change as you age, generally becoming longer as you progress towards menopause. Our bodies are sensitive to many outside factors too – your environment, general health, stress levels and lifestyle can all have an effect on your cycle. This is why a “one size fits all” approach to calculating your cycle and your fertility window doesn’t always work – it doesn't allow for the subtle variations in life and the adjustments your body makes in response.
When should I see someone about irregular periods?
The first thing to do is make sure your periods really are irregular and aren’t just fluctuating naturally. Tracking your cycle in an app or diary will give you a good picture of your health. One cycle isn’t enough information – it’s good to get at least 3 months’ data so you can start to identify patterns.
There may be an underlying health condition that’s affecting your cycle. You may wish to visit a healthcare professional if:
every month is different for you
your cycle is extremely short or long (less than 21 days or more than 35)
you have symptoms like gaining weight, being tired, hair growth on your face and dry or oily skin
you are struggling to get pregnant
Track periods to understand your cycle
The best way to become in tune with your hormones is to track your cycle (and moods and energy levels) using an app, or in your diary. You will soon start to see patterns forming and will figure out what phase you’re in, how you feel and how to adjust your activities to suit you best throughout the month.
No app or chart can always be 100% accurate; it’s always important to listen to your body and do what feels right. If your app or diary says one thing but you feel different, go with what your body is telling you. The female body is an incredible thing and understanding it brings you one step closer to feeling your best all month long.
Cycle syncing: Playing to your strengths
We all have times when it feels like we could take on the world and then days when even getting dressed seems like a challenge. Stress and lifestyle and outside events all have an impact on your get-up-and-go, but your cycle can also play a role.
The key is to work out when you are in each of the phases of your cycle, do more of the things your hormones support at that time, and do less of the things your hormones make more difficult at that time.
Hacking your cycle
Follicular, 1st half
Focus on Self-care
When it happens
Day 1 of your period is day 1 of your cycle. Periods can last anywhere between 2 and 7 days.
What happens to your hormones?
Low levels of oestrogen and progesterone can bring down your mood, and you may experience some mood swings. You might also feel some physical effects, like bloating and cramping.
How to make the most of it
Even though it may be the last thing you feel like, doing exercise in some form can really help during your period. When you’re feeling a bit flat, it’s tempting to reach for high-calorie treats to boost your mood, but junk food might actually end up making you feel worse. Think about some healthier alternatives for what you’re craving – fruit instead of sweets, for example, or wholegrain rather than white bread.
Follicular, 2nd half
Focus on taking on the world
When it happens
After your period, about day 7-14 of your cycle.
What happens to your hormones?
Levels of oestrogen, FSH and LH start to rise, giving you more energy and a better memory.
How to make the most of it
Use that energy and focus to take on important meetings or interviews, step up your workouts and explore creative projects. Your pain threshold is highest around now, so it’s a good time for a wax appointment!
Ovulatory
Focus on being the life and soul of the party
When it happens
In the middle of your cycle, around day 14.
What happens to your hormones?
Oestrogen peaks here, bringing with it positive, outgoing vibes. You might feel more sociable and confident, and many women experience a higher sex drive around the time of ovulation. It’s evolution’s way of keeping the species going!
How to make the most of it
This would be a great time to socialise and spend time with friends and loved ones as you’re at your happiest. Might also be a great time to plan a date night if you have a partner…
Luteal
Focus on cosy times
When it happens
After ovulation before the next period, around days 15-28.
What happens to your hormones?
Oestrogen, FSH and LH levels all fall, and progesterone rises. This helps prevent another egg being released, and prepares your body for either a pregnancy or a period. Progesterone can have a calming effect, but that can also mean you feel a bit down, with low libido, low energy and forgetfulness.
How to make the most of it
As your body prepares for your period, you may want to be a bit more gentle on yourself. It’s still beneficial to stay active though as exercise has been shown to improve PMS symptoms including mood and anxiety. Opt for exercises such as strength training, Pilates and yoga. This is usually a good time to rest and have some cosy evenings in.
The menstrual cycle is a (roughly) 28-day cycle controlled by female hormones.
The reason for the menstrual cycle is to prepare your body for a possible pregnancy. Your body goes through 4 phases each month, as an egg is released and is either fertilised (pregnancy) or broken down (a period). The timings of each phase differ slightly depending on what length cycle you have – cycle length can vary between women, and even month to month sometimes.
There are different levels of hormones interacting at each phase, and these can affect how you feel. Once you know what phase you’re in, you can work with your cycle to concentrate on activities that make the most of your mood, energy and general wellbeing.
The four phases of the menstrual cycle
In each phase of your cycle you’ll experience rising or falling levels of four hormones. Hormones are like messengers, and are sent from one part of the body to another to tell it what to do. There are dozens of hormones in the human body, but the ones that matter most for your cycle are:
Menstruation - day 1 (for up to a week)*
What’s happening?
Your uterus (womb) sheds its lining, and your Period starts. Periods usually last 3-7 days.
How do I feel?
As your hormones drop you may feel a little down or experience some mood swings.
Follicular Phase - days - 13/14*
What’s happening?
Your uterus lining is thickening ready to receive an embryo. This phase crosses over with the Menstruation phase. The hormone FSH stimulates follicles in the ovary to grow. Usually only one follicle will mature into an egg (around day 10).
How do I feel?
Once your period is over you may feel like you have more energy; your brain feels sharper and your memory is better. You might have a higher pain threshold.
Ovulation - Day 14 (roughly)*
What’s happening?
A mature egg is released from the ovary and travels along a fallopian tube towards your uterus. It survives for 24 hours and can be fertilised if it meets a sperm during this time.
How do I feel?
For many women their positive emotions and feeling peak during this phase, and so does their libido. Many women experience a higher sex drive during ovulation or at the end of this phase.
Luteal Phase - days 15-28*
What’s happening?
After ovulation progesterone is produced which thickens the uterus in preparation for pregnancy. If a fertilised egg implants into the uterus lining, this continues to be produced to maintain the thick uterus lining. If there is no embryo implanting, progesterone levels drop and the lining sheds, and your period starts.
How do I feel?
This is the phase you are most likely to experience PMS (premenstrual syndrome) symptoms such as mood swings and irritability. You may feel sluggish and absent-minded. Your sex drive may also drop, partly due to the high levels of progesterone, but also due to the other feelings you may be experiencing such as low mood or fatigue, which naturally makes you less interested in having sex!
*Timings differ depending on the length of the cycle
What is the ‘fertility window’?
The fertility window includes the days around ovulation where your chances of getting pregnant are highest. If you’re looking to conceive, it makes sense to time intercourse to fit in with your fertile window. Equally, if you do not want to get pregnant but are having regular sex with a male partner, it’s worth knowing when you both may need to be extra careful with your contraception.
Did you know?
It’s a myth that you can get pregnant at any point in your cycle. What IS true is that every woman is different, and each cycle is different, so it’s difficult to predict exactly when your fertile window will be.
What if I have irregular periods?
First off – you’re not alone. Many women experience cycles that change from month to month, and it’s estimated only 13% of women have a 28-day cycle. It’s completely normal to have cycles ranging from 25 to 30 days.
Your cycles can also change as you age, generally becoming longer as you progress towards menopause. Our bodies are sensitive to many outside factors too – your environment, general health, stress levels and lifestyle can all have an effect on your cycle. This is why a “one size fits all” approach to calculating your cycle and your fertility window doesn’t always work – it doesn't allow for the subtle variations in life and the adjustments your body makes in response.
When should I see someone about irregular periods?
The first thing to do is make sure your periods really are irregular and aren’t just fluctuating naturally. Tracking your cycle in an app or diary will give you a good picture of your health. One cycle isn’t enough information – it’s good to get at least 3 months’ data so you can start to identify patterns.
There may be an underlying health condition that’s affecting your cycle. You may wish to visit a healthcare professional if:
every month is different for you
your cycle is extremely short or long (less than 21 days or more than 35)
you have symptoms like gaining weight, being tired, hair growth on your face and dry or oily skin
you are struggling to get pregnant
Track periods to understand your cycle
The best way to become in tune with your hormones is to track your cycle (and moods and energy levels) using an app, or in your diary. You will soon start to see patterns forming and will figure out what phase you’re in, how you feel and how to adjust your activities to suit you best throughout the month.
No app or chart can always be 100% accurate; it’s always important to listen to your body and do what feels right. If your app or diary says one thing but you feel different, go with what your body is telling you. The female body is an incredible thing and understanding it brings you one step closer to feeling your best all month long.
Cycle syncing: Playing to your strengths
We all have times when it feels like we could take on the world and then days when even getting dressed seems like a challenge. Stress and lifestyle and outside events all have an impact on your get-up-and-go, but your cycle can also play a role.
The key is to work out when you are in each of the phases of your cycle, do more of the things your hormones support at that time, and do less of the things your hormones make more difficult at that time.
Hacking your cycle
Follicular, 1st half
Focus on Self-care
When it happens
Day 1 of your period is day 1 of your cycle. Periods can last anywhere between 2 and 7 days.
What happens to your hormones?
Low levels of oestrogen and progesterone can bring down your mood, and you may experience some mood swings. You might also feel some physical effects, like bloating and cramping.
How to make the most of it
Even though it may be the last thing you feel like, doing exercise in some form can really help during your period. When you’re feeling a bit flat, it’s tempting to reach for high-calorie treats to boost your mood, but junk food might actually end up making you feel worse. Think about some healthier alternatives for what you’re craving – fruit instead of sweets, for example, or wholegrain rather than white bread.
Follicular, 2nd half
Focus on taking on the world
When it happens
After your period, about day 7-14 of your cycle.
What happens to your hormones?
Levels of oestrogen, FSH and LH start to rise, giving you more energy and a better memory.
How to make the most of it
Use that energy and focus to take on important meetings or interviews, step up your workouts and explore creative projects. Your pain threshold is highest around now, so it’s a good time for a wax appointment!
Ovulatory
Focus on being the life and soul of the party
When it happens
In the middle of your cycle, around day 14.
What happens to your hormones?
Oestrogen peaks here, bringing with it positive, outgoing vibes. You might feel more sociable and confident, and many women experience a higher sex drive around the time of ovulation. It’s evolution’s way of keeping the species going!
How to make the most of it
This would be a great time to socialise and spend time with friends and loved ones as you’re at your happiest. Might also be a great time to plan a date night if you have a partner…
Luteal
Focus on cosy times
When it happens
After ovulation before the next period, around days 15-28.
What happens to your hormones?
Oestrogen, FSH and LH levels all fall, and progesterone rises. This helps prevent another egg being released, and prepares your body for either a pregnancy or a period. Progesterone can have a calming effect, but that can also mean you feel a bit down, with low libido, low energy and forgetfulness.
How to make the most of it
As your body prepares for your period, you may want to be a bit more gentle on yourself. It’s still beneficial to stay active though as exercise has been shown to improve PMS symptoms including mood and anxiety. Opt for exercises such as strength training, Pilates and yoga. This is usually a good time to rest and have some cosy evenings in.
Your experience matters. Has this content been helpful?
Share your answer to see how others responded.
Your answers will help us to ensure our content is useful for people who want to learn more about fertility and reproductive choices.
Do you feel more informed about fertility?
Yes
76%
No
24%
Before discovering our content, what did you believe was the primary cause of fertility issues?
Poor diet
34%
Excessive consumption of alcohol
19%
Smoking
16%
Age
21%
Other
9%
Since learning more, what do you now believe is the main cause of fertility issues?
Poor diet
36%
Excessive consumption of alcohol
14%
Smoking
11%
Age
39%
Since learning more, what will you do now?
Use knowledge for informed decisions
47%
Consider altering future plans
24%
Consider talking with a fertility specialist
12%
Book an appointment with a fertility specialist
17%
How old are you?
<25 years
29%
26-30 years
22%
31-35 years
17%
36-40 years
11%
>40 years
21%
References
American Society for Reproductive Medicine. Optimizing natural fertility: a committee opinion. Fertility and Sterility. 2017;107(1):52-58.
Bull JR, et al. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. npj Digital Medicine. 2019;2:83. Available at: https://doi.org/10.1038/s41746-019-0152-7. Last accessed: July 2024.